
Root Planing
Conservative treatment to eliminate the need for gum surgery
Dear Doctor,
I went to my dentist recently after an absence of about three years. I was told I had early periodontal disease with pockets of 5 to 6mm around my back teeth and that I needed root planing. Can you tell me what root planing is and what it does?
Dear Harold,
Deep cleaning or root planing is a very routine dental procedure for the preliminary treatment of periodontal (peri-around, odont-tooth) disease.
A little background will be helpful in understanding what this common procedure is and does. Of the different forms of periodontal disease, most are caused by biofilms of dental (bacterial) plaque sticking and adhering to the teeth around the gum line in the absence of good oral hygiene. If left unremoved, the bacteria in the plaque can cause inflammation of the gums, and further progression (in some people) will cause loss of attachment of the gum tissues to the teeth resulting in pocket formation. This is just like a pocket in your clothing into which you can insert your hand, except your dentist will measure the degree of vertical detachment with a periodontal probe generally marked in millimeters. Once bacterial plaque penetrates into these pockets they become pathogenic (disease causing), and further inflammation and infection can lead to bone loss, tooth loosening, abscess formation and ultimately tooth loss.
 |
 |
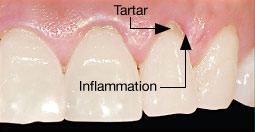
| The top photograph shows gum tissue inflammation and the presence of tartar below the gum tissue. In the bottom photograph the tartar has been removed by scaling and root planing returning the gum tissue to health. |
Bacteria and their breakdown products damage the fine structure of the root surfaces by becoming ingrained into them so that a preliminary phase of treatment must include removal of these products and toxins. Bacterial products on the root surfaces also calcify and stick to them; these hard deposits commonly known as tartar or calculus are just like the ones which most commonly form behind the lower front teeth.
Basic treatment of almost all types of periodontal disease includes both oral hygiene education and training to ensure that you can remove plaque daily as it rebuilds, and before it progresses into the pockets. Removal of bacteria from diseased root surfaces will allow the gum tissues to begin to heal. This is where root planing comes in. In addition to scaling (removal of the more superficial collections of calculus), root planing as the name implies actually involves physically planing the roots. This procedure removes subgingival (sub-beneath, ginigival-gums) calculus, bacteria, and toxins ingrained into the root surfaces allowing the periodontal (gum) tissues to heal.
Root planing procedures are generally best carried out with local anesthesia (numbing the teeth and surrounding soft tissues) to allow the hygienist, dentist or periodontist to meticulously clean the root surfaces in an efficient and comfortable manner. Local anesthesia is a really good idea, since as we say in dentistry, “the most important piece of calculus is the last piece,” usually deep at the base of the pockets, and gum tissues are sensitive. It is rather common for the dental professional who is doing the cleaning to first use an ultrasonic device, generally an instrument that cleans by vibrating particles off the root surfaces and simultaneously flushes the pockets out with water. The root planing is then finished with delicate small hand instruments known as curettes. It is not uncommon to further irrigate the pockets with an antibacterial medication like iodine, chlorhexidene or in some specific cases, antibiotics.
Root planing is indeed a delicate procedure which requires experience and finesse depending largely upon tactile (feeling) ability of the clinician, since without surgery one cannot see within the pockets. An experienced clinician will know when a properly cleaned root surface has been achieved, not only by feel, but also by an ability to “read the gum tissues” which will change color ever so slightly when all the deposits have been removed.
Pocket or probing depth is important and can be used as a guideline to success in this endeavor. Multiple studies over the years have shown that at pocket depths up to 3-5mm successful cleaning is quite predictable, from 5-7 mm the chances are about 50/50 and greater than 7mm the chances of leaving deposits remain. This is an over simplification since many other factors are involved like the degree of gum swelling and infection, as well as the difficulty imposed by the shapes and configurations of the roots.
It is important to know that it is sometimes not possible to remove all the deposits at one sitting for the above mentioned reasons, so that coming back to the same area a few weeks later may allow for some refinement in removing remaining deposits. The outcome of root planing will be affected by the degree of daily plaque control, the better the daily plaque removal the better the gum tissue healing response and the easier to remove deposits. As the gum tissues heal there is less inflammation and bleeding so that subsequent removal of root surface deposits becomes easier.
The response to root planing or “initial” periodontal therapy as it is known is usually evaluated three to four weeks following the procedure when gum tissue healing is reviewed and probing measurements are retaken. It is not uncommon for inflamed tissues to heal by 1-3 mm, sometimes returning the tissues to complete health with root planing alone.
After root planing, patients may experience some tooth sensitivity to hot and cold, particularly if there is pre-existing gum tissue recession. This is usually treated with the application of fluoride to the root surfaces. Some minor sensitivity of the gum tissues themselves is also common, but can usually be managed by minor non-steroidal analgesic (pain) and anti-inflammatory medication like tylenol, aspirin or ibuprofen.